General information on the 4AT
What is the 4AT?
The 4AT is a quick clinical assessment tool for delirium and cognitive impairment. It was developed in 2011 to provide a rapid clinical assessment that healthcare staff can use at the bedside. Since its development, it has become the most-validated delirium assessment tool in the literature, and it is in global use.
A particular strength of the 4AT is that not only does it have very strong validation data, it has multiple large scale studies showing that it is effective in routine clinical practice.
What does the 4AT acronym stand for?
The “4” refers to the four components of the test (Alertness, AMT4, Attention, Acute Change/Fluctuating Course, and “AT” stands for Assessment Test.
What are the key features of the 4AT?
-
Rapid: Takes less than 2 minutes to complete.
-
Simple: No special training required for administration.
-
Inclusive: Can be used in patients unable to provide verbal responses or those with sensory impairment; includes scoring for ‘untestable’ patients, avoiding ‘Unable to Assess’ results common with some other tools.
-
Evidence-Based: Validated in numerous studies across various settings.
-
Widely Recommended: Included in multiple international clinical guidelines.
-
Free Access: Available for free download and use, including integration into EHR/EMR systems, without permission or registration.
Who developed the 4AT and when?
The 4AT was developed by a multidisciplinary team led by Prof. Alasdair MacLullich at the University of Edinburgh, UK. The first version was created in 2011, with the current Version 1.2 released in 2014. It was developed to address the need for a practical, usable delirium assessment tool that could be used without special training in busy clinical environments.
What is the target population for the 4AT?
The 4AT is designed for use in adults (≥18 years) in all clinical settings, including emergency departments, medical and surgical wards, ICU, rehabilitation units, and nursing homes. It is particularly recommended for use in older adults (≥65 years) who are at higher risk of delirium. The 4AT is not validated for use in children or adolescents.
Is the 4AT free to use? Do I need permission or registration?
The 4AT is completely free to use.
No permission, payment, or registration is required. The 4AT is made freely available under the CC BY 4.0 licence, meaning it can be used, reproduced, and adapted with appropriate attribution.
For reproductions or adaptations, please use the following attribution:
4AT © 2011–2014 Alasdair MacLullich, Tracy Ryan and Helen Cash.
Licensed under CC BY 4.0.
Official and current version: https://www.the4at.com.
No warranty is given as to accuracy or fitness for purpose.
Full attribution and reuse instructions, including how to label translations and other modified versions, are on the Attribution and reuse page.
The developers encourage widespread use to improve delirium detection and care.
What guidelines include the 4AT?
The 4AT is included in multiple national and international clinical guidelines, for example:
-
UK NICE Guidelines on Delirium (2023; replaced the CAM)
-
Scottish Intercollegiate Guidelines Network (SIGN) Delirium Guidelines (2019)
-
European Society of Anaesthesiology and Intensive Care (ESAIC) Guidelines on Postoperative Delirium (2017)
-
Australian Delirium Clinical Care Standard (2021)
-
American Psychiatric Association Practice Guideline on Delirium (2023)
-
The 4AT is also included in many local hospital protocols worldwide.
Scoring & Interpretation
What do the different 4AT scores mean?
The 4AT provides a score from 0-12 that is interpreted in three categories:
-
0: Delirium or severe cognitive impairment unlikely (but delirium still possible if information incomplete)
-
1-3: Possible cognitive impairment; more detailed cognitive testing and/or informant history-taking advised
-
4 or above: Possible delirium +/- cognitive impairment.
A score of 4 or above indicates possible delirium and should prompt clinical assessment. The 4AT is a well-validated, reliable tool for detecting delirium, suitable for routine use at scale. Its result is interpreted in the overall clinical context, as for every clinical assessment tool.
How is Item 1 (Alertness) scored?
This item assesses the patient’s level of alertness at the time of assessment, through observation.
-
Score 0: Normal alertness (fully alert and not agitated) OR mild sleepiness lasting less than 10 seconds after waking, then normal.
-
Score 4: Clearly abnormal alertness. This includes being markedly drowsy (e.g., difficult to rouse, obviously sleepy during assessment) OR agitated/hyperactive.
Guidance: Observe the patient throughout the assessment. If asleep, attempt to wake them with speech or a gentle touch. Asking their name and address can aid assessment. Altered alertness is a strong indicator of delirium in hospital settings.
How is Item 2 (AMT4) scored?
The AMT4 (Abbreviated Mental Test – 4) is a brief cognitive test comprising four questions:
-
1. Age
-
2. Date of birth
-
3. Place (name of the hospital or building)
-
4. Current year
It is a shortened version of the original 10-item Abbreviated Mental Test.
A score of 0 indicates all answers were correct, 1 indicates one error, and 2 indicates two or more errors or if the patient is untestable.
How is Item 3 (Attention) scored?
This item assesses attention using the Months Backwards test. Ask the patient: “Please tell me the months of the year in backwards order, starting at December.” One initial prompt (“What is the month before December?”) is allowed.
-
Score 0: Achieves 7 or more months correctly (i.e., recites backwards correctly to June)
-
Score 1: Starts the test but recites fewer than 7 months correctly OR refuses to start
-
Score 2: Untestable (cannot start the test because they are too unwell, drowsy, or inattentive)
How is Item 4 (Acute Change or Fluctuating Course) scored?
This item assesses evidence of an acute change OR fluctuation in alertness, cognition (e.g., new confusion, disorientation), or other mental function (e.g., paranoia, hallucinations) over the last 2 weeks, which is still present in the last 24 hours. This information usually comes from sources like staff, carers, family, notes, or your own knowledge of the patient.
-
Score 0: No evidence of acute change or fluctuation.
-
Score 4: Evidence of acute change or fluctuation is present.
Guidance: Asking collateral sources or the patient about recent changes in confusion, sleep patterns, or unusual experiences can help. Marked fluctuation strongly suggests delirium. This item incorporates the concept of the ‘Single Question in Delirium’ (SQiD).
What if a patient is unable to complete parts of the 4AT?
One of the key advantages of the 4AT is its ability to assess patients who cannot undergo cognitive testing due to drowsiness, agitation, or other reasons:
• For Item 1 (Alertness): If the patient has abnormal alertness (drowsy, agitated, etc.), they score 4 points.
• For Item 2 (AMT4): If the patient cannot be assessed (e.g., too drowsy), score as “untestable” = 2 points.
• For Item 3 (Attention): If the patient cannot be assessed, score as “untestable” = 2 points.
• For Item 4 (Acute Change): This can often still be completed by obtaining information from caregivers or records.
This design ensures that patients who cannot be assessed (who are at high risk of delirium) will generally score 4 or above, triggering appropriate clinical assessment. This is a major advantage over tools that cannot be scored if the patient cannot communicate.
Evidence & Validation Studies on the 4AT
Is the 4AT a validated tool?
Yes, the 4AT is rigorously validated. Its diagnostic accuracy has been assessed in 31 published studies, encompassing more than 6,000 patients across diverse international clinical settings. The 4AT has the largest diagnostic test accuracy evidence base of any delirium assessment tool.
What studies support its use?
The evidence base includes the initial validation study in geriatric inpatients, numerous subsequent studies in settings like emergency departments, acute medical and surgical wards, stroke units, oncology, and palliative care, and multiple systematic reviews and meta-analyses that pool data from these studies. Key references are available here.
What is the sensitivity and specificity of the 4AT?
A major meta-analysis by Tieges et al. (2021) including 17 studies (3,702 observations) found a pooled sensitivity of 0.88 (95% CI 0.80–0.93) and a pooled specificity of 0.88 (95% CI 0.82–0.92).
The 4AT now has an even larger body of validation studies (31 studies with >6000 patients), with results broadly aligned with the above meta-analysis.
Practical Use & Clinical Implementation
How long does the 4AT take to administer?
The 4AT is designed for rapid assessment and usually takes less than 2 minutes to complete in routine clinical practice.
Is specific training required to use the 4AT?
No. A key design feature of the 4AT is that it does not require specific training courses or certification for its use. It was developed for straightforward application by a wide range of healthcare staff (doctors, nurses, therapists, etc.) as part of their routine assessment. Familiarity with the items and scoring can be achieved by reviewing the tool, the user guide and the 4AT case examples.
How often should the 4AT be used?
The 4AT is best used as an episodic assessment tool rather than for continuous high-frequency monitoring. Recommended times for use include:
-
At initial hospital admission or presentation (e.g., in the Emergency Department or admission unit).
-
Before and after surgery (perioperatively).
-
During transitions of care between wards or facilities.
-
Whenever delirium is suspected based on clinical observation or changes in the patient’s condition.
-
Following a positive screen on a brief monitoring tool (e.g., SQiD, NuDESC).
-
Periodically (e.g., once daily) to track recovery from an episode of delirium.
Using the 4AT multiple times per day for extended periods solely for monitoring purposes is generally discouraged due to potential burden on patients and staff.
Can the 4AT be used in different clinical settings?
Yes, the 4AT is versatile and has been validated and implemented in numerous clinical settings, including: Emergency Departments, acute medical and surgical wards, geriatric and rehabilitation units, stroke services, oncology units, palliative care settings (including hospices), and care homes.
Can the 4AT be used in the Intensive Care Unit (ICU)?
The 4AT was primarily developed and validated for non-ICU settings. For patients in the ICU, especially those who are mechanically ventilated, tools specifically designed for that environment, such as the CAM-ICU (Confusion Assessment Method for the ICU) or the ICDSC, are the standard recommended tools. While one recent study explored the 4AT in critically ill patients and found acceptable performance compared to CAM-ICU, current guidelines generally recommend CAM-ICU or ICDSC for routine ICU delirium assessment.
How should administration be adapted for patients with communication difficulties?
It’s essential to consider communication challenges like hearing or visual impairment, dysphasia, or language barriers.
Ensure optimal conditions: use hearing aids, glasses; ensure good lighting; minimize background noise; use interpreters if needed.
Speak clearly and allow adequate time for responses.
The 4AT’s combination of sources of information: observation (Item 1) and collateral history (Item 4), plus its ability to score cognitive items as ‘untestable’ (Items 2 & 3), makes it more adaptable than some purely interview-based tools. If direct cognitive testing is impossible, the ‘untestable’ scoring ensures an assessment can still be completed. Collateral information for Item 4 becomes even more valuable in these situations.
Can the 4AT be used in patients with known dementia?
Yes, the 4AT is suitable for use in patients with dementia and has been validated in cohorts including individuals with pre-existing cognitive impairment.
-
Delirium Detection: It helps identify delirium superimposed on dementia, which is common but challenging to diagnose. Good sensitivity is maintained in this group.
-
Specificity Consideration: In patients with severe dementia, specificity might be reduced. This is because profound baseline cognitive impairment could lead them to score points on Items 2 and 3 even without active delirium, potentially resulting in a score of 4.
-
Clinical Approach: A 4AT score of 4+ in someone with dementia warrants assessment for delirium. Differentiating delirium from underlying dementia requires careful clinical evaluation, focusing on acute changes from the patient’s baseline mental state (Item 4 is key) and utilising informant history whenever possible. The diagnosis remains clinical.
-
The 4AT score range indicates cognitive impairment and can be used as an indicator of possible dementia (study).
Is the 4AT available in other languages?
Yes, the 4AT has been translated into many languages to support its international use. Available translations include Italian, German, Spanish, Portuguese, Danish, French, Icelandic, Norwegian, Arabic, Finnish, Czech, Dutch, Polish, Swedish, Chinese, Turkish, Korean, Thai, Russian, Hebrew, and Japanese. Validated versions exist for several languages. You can find links to available translations here.
Can the 4AT be integrated into Electronic Health Records (EHR/EMR)?
Yes. The 4AT is free to incorporate into EHR/EMR systems without licensing fees or specific permission. Many hospitals and healthcare systems have successfully embedded the 4AT into their digital platforms to facilitate routine assessment, documentation, and data collection for quality improvement and research.
What evidence supports implementation of the 4AT in the real world?
The 4AT has been studied in multiple large scale datasets, and generally shows high uptake and positive score rates aligned with the expected rates of delirium. See here for a list of implementation studies.
Comparisons of the 4AT with Other Tools
How does the 4AT compare to the Confusion Assessment Method (CAM)?
The CAM is a well-established tool for delirium identification. The 4AT was developed later, aiming for greater brevity and ease of use in routine practice. Here’s a comparison based on key practical features and evidence:
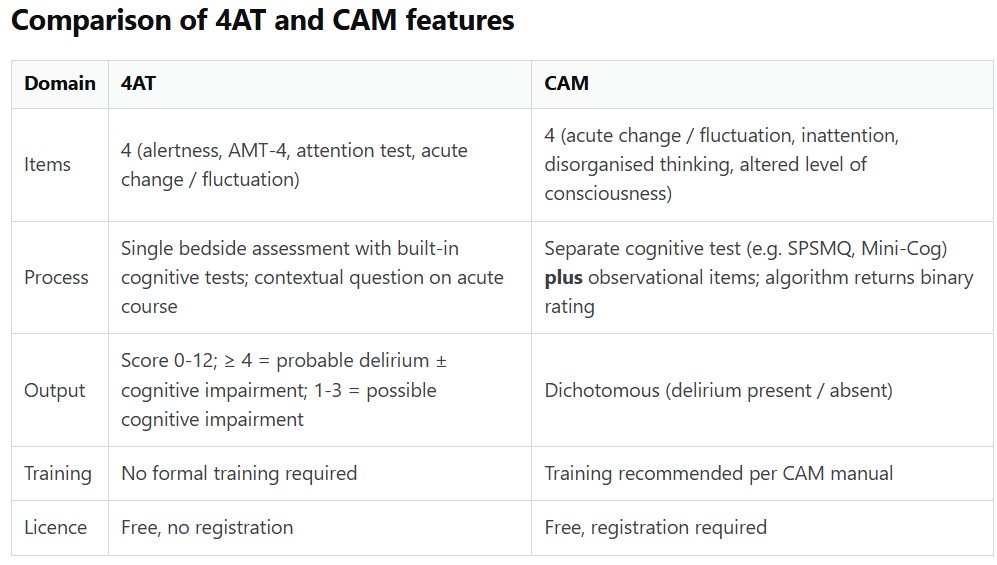
The 4AT takes 2 mins, and the CAM takes 5 minutes. The 4AT incorporates cognitive tests and the CAM requires a separate cognitive test to be done before the CAM is scored. The 4AT provides a score range with three categories including no delirium, cognitive impairment but no delirium, and delirium; the CAM provides a delirium yes or no binary classification. The 4AT does not require training; the CAM does require training and studies show that the CAM has lower sensitivity if done by staff without training.
In large-scale, high quality RCT, the 4AT showed higher sensitivity and similar specificity to the CAM.
Importantly, there is an unofficial, unvalidated version of the CAM that does not involve cognitive testing; this is shorter than the original CAM but the evidence shows that this unofficial version (termed the CAM-Lite in a blog describing this issue) has low sensitivity for delirium in practice.
Summary: the original CAM works if performed by trained staff who do the essential preceding cognitive test. However, the 4AT works well in staff without special training, and has built-in cognitive tests. The 4AT is also faster than the CAM. This means that the 4AT is more suited to implementation in the real world. A non-expert can apply the 4AT in under 2 minutes and detect delirium; whereas non-experts often struggle to apply CAM correctly in a busy setting.
Overall, because it has similar psychometric performance, a much larger diagnostic test accuracy study evidence base, faster speed, better usability in practice, higher sensitivity in practice, and does not need special training, the 4AT is now broadly considered to be a superior tool to the CAM for routine clinical use. It is replacing the CAM in many hospitals across the world now, including in the United States of America and Canada.
How does the 4AT compare to the Brief CAM (bCAM)
The bCAM uses the CAM algorithm (requiring Feature 1: Acute Change/Fluctuation and Feature 2: Inattention, plus either Feature 3: Altered LoC or Feature 4: Disorganised Thinking).
It uses built-in, specific tests for inattention.
Time: Both 4AT and bCAM are designed to be rapid (<2 minutes).
Validation: bCAM has shown good sensitivity (78%-84%) and very high specificity (96%-97%) in ED validation studies. The 4AT has demonstrated sensitivity and specificity around 88% in pooled analyses across many settings, including
Training: 4AT requires no specific training. While bCAM is designed to be brief, effective use of CAM-based tools often benefits from training on assessing the core features.
Summary: bCAM offers a quick, CAM-based assessment with high specificity. The 4AT provides a similarly rapid assessment with robust validation across more studies and settings.
Both tools offer built-in cognitive testing, though the 4AT offers a scoring range with three categories of outcomes and the bCAM gives a binary outcome.
How does the 4AT compare to the 3D-CAM?
Validation: 3D-CAM showed good sensitivity (95%) and specificity (94%) in its main validation study. The 4AT has been validated in more studies (31) across a wider range of clinical settings than the 3D-CAM.
The 3D-CAM is a well-validated, structured CAM-based tool with good accuracy.
The 3D-CAM operationalises the Confusion Assessment Method (CAM). Twenty yes/no prompts, read from a template, are completed and entered into an algorithm that labels delirium present/absent.
The 3D-CAM takes 3 minutes, 1 minute longer than the 4AT. The 3D-CAM requires training. The 4AT offers similarly robust performance with advantages in speed and simplicity (no training needed). The 4AT has a broader evidence base across diverse settings, with more real world implementation data.
How does the 4AT compare to the Ultra-Brief CAM (UB-CAM)?
UB-CAM is a two-stage test that starts with 2 cognitive test items, then if either answer is wrong, the 3D-CAM is completed with some modifications designed to shorten the process. The overall time for completion of the UB-CAM is similar to the 4AT. The tools have broadly similar sensitivity and specificity.
The UB-CAM requires training while the 4AT requires no special training.
Both the UB-CAM and the 4AT offer built-in cognitive testing, though the 4AT offers a scoring range with three categories of outcomes and the UB-CAM gives a binary outcome.
The 4AT has a larger evidence base than the UB-CAM, with substantially more real world implementation data.
How does the 4AT compare to the NuDESC?
NuDESC is an observational tool based on nursing assessments over a shift, designed to be used for ongoing monitoring. Five behaviours are assessed and scored 0–2, total 0–10; ≥2 suggests delirium.
The NuDESC does not involve direct cognitive testing like the 4AT.
The NuDESC has lower sensitivity to 4AT though similar specificity but lower specificity than CAM.
The 4AT needs no training. Some training is required for the NuDESC.
Summary: NuDESC is a nursing observation tool for ongoing monitoring. The 4AT is designed more for episodic use.
How does the 4AT compare to DOSS?
DOSS is a monitoring tool suitable for ongoing checks, while the 4AT is a tool best used at specific time points (admission, suspected change). A positive DOSS screen might prompt a 4AT assessment.
Validation: DOSS has shown variable sensitivity (reported range 25%-97%) and good specificity (89%-98%) in reviews. The 4AT demonstrates consistent pooled sensitivity and specificity around 88% across a larger number of validation studies.
How does the 4AT compare to the Single Question in Delirium (SQiD)?
The SQiD involves one informant question: “Is the patient more confused [or drowsy] than usual?”
The SQiD is an ultra-brief tool which if positive should trigger a more definitive assessent such as the 4AT. Used together they balance speed and diagnostic certainty in everyday busy clinical settings.
Summary: what are the key advantages of the 4AT delirium assessment tool?
-
Speed and Simplicity: Quick administration (<2 mins) without needing special training makes it easy to integrate into busy workflows.
-
Inclusivity: The ability to score ‘untestable’ patients ensure assessment completion for everyone, including drowsy or noncommunicative individuals.
-
Leading Formal Validation Data: The 4AT is the world’s leading delirium tool in terms of formal validation data, and the validation data spans the widest range of settings.
-
Leading Clinical Implementation Data: In addition to leading validation data, the 4AT also has the largest body of published clinical implementation data (example) of any delirium tool.
-
Guideline Recommended: Endorsement in multiple major clinical guidelines.
-
Can be used to assist in dementia assessment.
-
Formally validated as a tool to assess recovery from delirium.